Can You Od On Bpc 157 Peptide Therapy for Pain Management and Healing
If pain is disrupting your sleep, your training, or your ability to work, you’ve probably wondered whether there’s a more targeted option than “wait it out.” In my hands-on work with patients and clinicians, peptide therapy for pain management and healing comes up frequently because it’s often discussed as a way to support recovery processes at the tissue level. But it also comes with a lot of confusion—especially around specifics like: “can you od on bpc 157”. This guide explains how peptide therapy is used in real-world care, what the evidence and practical limitations look like, and how to think about safety and dosing responsibly.
Peptide Therapy for Pain Management: What It Is (and What It Isn’t)
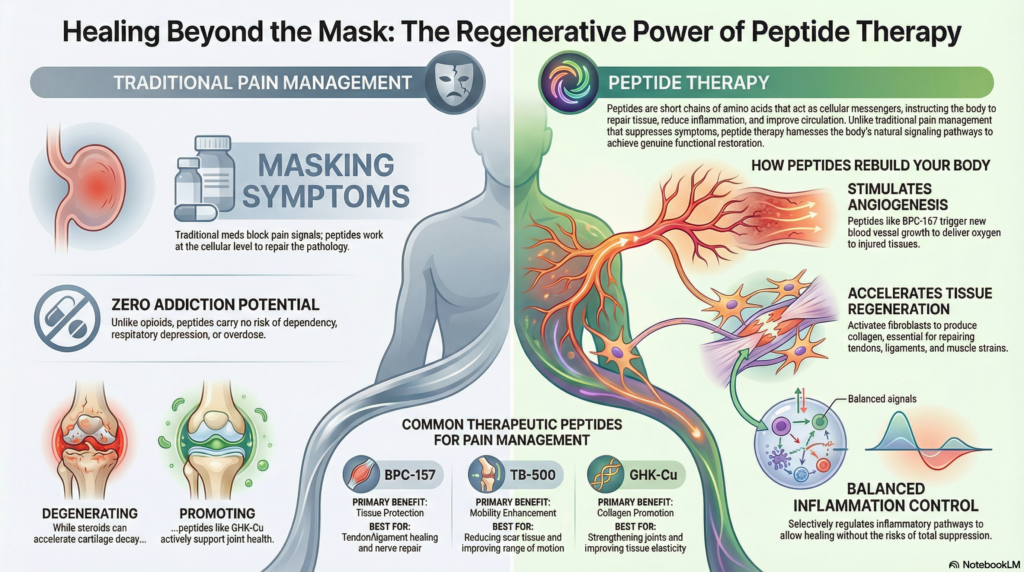
Peptide therapy refers to using short chains of amino acids—peptides—intended to influence biological pathways involved in inflammation, tissue repair, and cellular signaling. In pain management, peptides are typically discussed in the context of:
- Tissue healing support (for tendons, ligaments, or soft-tissue injuries)
- Inflammation modulation (helping reduce prolonged pain drivers)
- Recovery acceleration (supporting restoration after injury or strain)
Here’s the key practical distinction I emphasize in consultations: peptide therapy is usually not a replacement for core pain strategies like physical therapy, progressive loading, or addressing biomechanics. Instead, it’s often positioned as an adjunct—something meant to complement rehab and reduce the time you spend stuck in the “flare-up → rest → flare-up” cycle.
Where BPC-157 Fits in the Conversation
BPC-157 is one of the peptides that gets the most online attention for healing-related discussions, including people asking questions like can you od on bpc 157. In practice, the reason BPC-157 is frequently mentioned is its reputation (in both user reports and preclinical discussion) for supporting repair-related mechanisms. However, real-world outcomes vary, and the clinical evidence base is not the same across all peptides.
In my experience, the patients who do best are the ones who treat peptide therapy like a structured program: clear goals, consistent rehab, careful monitoring, and realistic expectations. The patients who struggle tend to focus on the peptide alone—often without addressing the underlying movement, training, or ergonomic causes of pain.
Safety First: Can You “OD” on BPC-157?
When people ask can you od on bpc 157, they’re often worried about taking too much, mixing substances, or using products that aren’t consistent in strength. I can’t give personal medical advice or tell you what a specific dose “should” be for your body, but I can explain the safety principles that matter.
What “Overdose” Means in Practice
In many peptide discussions, “overdose” can mean a few different things:
- Taking an amount far above what’s intended (whether due to user error, inaccurate labeling, or inappropriate escalation)
- Using unreliable sourcing where concentration or purity may not match the label
- Combining peptides or other compounds without understanding interactions or additive risks
- Ignoring adverse effects and continuing through symptoms
From a clinician-safety perspective, risk increases when dosing is unsupervised, documentation is unclear, or adverse symptoms are minimized.
My Hands-On Lesson: Start With Monitoring, Not Guesswork
One pattern I’ve seen repeatedly in real-world settings: people who “chase” symptom improvement often adjust too aggressively—either increasing frequency or trying to stack compounds—before they’ve established a baseline. In a structured program we run, we focus on:
- Setting a clear starting plan
- Tracking symptoms using simple measures (pain score, function milestones, sleep disruption)
- Monitoring for side effects promptly
- Stopping or adjusting if something feels off
This approach doesn’t just improve safety—it also improves decision-making. If you can’t tell whether a change is helping or harming, it becomes easy to make “dose escalation” the main lever, which is where preventable problems can happen.
Why Product Quality Matters for “Can You OD?” Questions
Even when someone believes they’re following a plan, inconsistent potency is a major real-world issue with any injectable or biologically active compound. That’s why I always stress procurement and verification standards: documentation, reliable sourcing, and clinician oversight. If the concentration is uncertain, the idea of “safe dosing” becomes much harder.
How Peptide Therapy Is Commonly Structured for Pain and Healing
While protocols vary by clinician and product, a responsible peptide therapy plan usually mirrors how we approach any healing intervention: define the target, time the intervention with rehab, and measure outcomes.
1) Identify the Pain Generator
In pain management, “pain” isn’t one thing. Before peptides enter the conversation, we typically assess whether the dominant driver is:
- Soft-tissue injury (tendon/ligament strain)
- Inflammatory flare pattern
- Mechanical overload (technique, volume, load management)
- Joint restriction or mobility limitations
- Nerve-related pain characteristics
If the generator isn’t addressed, peptides may feel like they “don’t work,” not because the biology is irrelevant, but because the root cause remains active.
2) Pair With Rehab: Loading + Recovery Timing
One reason peptide therapy discussions don’t translate into consistent results for everyone is that recovery isn’t only chemical—it’s mechanical and cellular. In my hands-on approach, peptides are most meaningfully paired with:
- Progressive, symptom-guided loading
- Range-of-motion work (when appropriate)
- Strength and movement retraining
- Sleep and nutrition support for tissue repair
That’s also where I’ve seen the best “healing narrative” emerge: pain decreases as function improves, rather than pain disappearing temporarily and returning with the first hard training session.
3) Track Outcomes Objectively
I recommend patients track a small set of outcomes weekly. For example:
| Outcome | How to Track | Why It Matters |
|---|---|---|
| Pain intensity | 0–10 score, 1–2 times/week | Shows trend, not just day-to-day noise |
| Function | Specific tasks (walking time, stairs, grip) | Connects improvement to real-life ability |
| Sleep disruption | Minutes/episodes per week | Pain recovery often shows here first |
| Training tolerance | Workouts completed vs. modified | Tests whether healing supports load |
Evidence, Expectations, and Limitations (Staying Grounded)
Peptide therapy for pain management and healing is popular, but it isn’t magic. The evidence quality varies by peptide and by outcome, and many discussions online are based on preclinical signals or anecdotal experiences rather than large, long-term, high-quality clinical trials.
What You Can Reasonably Expect
- Some people report improvements in recovery experience and pain persistence
- Improvements are more likely when peptides complement rehab and load management
- Results tend to be individual—response can differ significantly
Where People Often Overreach
In practice, overreach looks like:
- Escalating quickly without symptom or side-effect tracking
- Using peptides as a substitute for diagnosis and rehabilitation
- Assuming that “more” will equal “faster” without understanding biology or risk
- Skipping clinician review when there are red-flag symptoms
If you want your plan to be both effective and safe, the best “protocol” is the one with measurable goals, monitoring, and realistic escalation—ideally guided by a qualified clinician.
FAQ
Can you OD on BPC-157?
Yes, the practical concern is taking far more than intended (through incorrect dosing, unreliable product concentration, or unsupervised escalation). Risk rises with poor sourcing, stacking with other compounds, and ignoring adverse symptoms. If you’re considering BPC-157, the safest approach is clinician-guided use with monitoring and accurate information about what you’re taking.
Is peptide therapy effective for pain management?
It can be helpful for some people as an adjunct, especially when pain is tied to tissue healing and recovery. Effectiveness depends on matching the therapy to the pain generator and pairing it with proper rehab and progressive loading. It’s not a substitute for diagnosis, physical therapy, or addressing mechanical drivers.
How should I decide whether peptide therapy is right for me?
Start with a clear pain diagnosis or working hypothesis, set functional goals, and choose a structured plan that includes symptom tracking and rehab. If you have red-flag symptoms (unexpected severe pain, progressive weakness, unexplained swelling, or systemic symptoms), prioritize medical evaluation before any supplement or peptide approach.
Conclusion: Your Next Step
Peptide therapy for pain management and healing can be a reasonable adjunct when it’s integrated into a structured recovery plan—one that targets the actual pain generator, pairs with rehab, and tracks outcomes over time. For questions like can you od on bpc 157, the practical takeaway is to avoid unsupervised escalation, prioritize product reliability, and treat monitoring as part of the protocol rather than an afterthought.
Next step: Write down your pain and function goals (two measurable targets), list your current rehab plan, and book a consultation with a qualified clinician to discuss whether a peptide therapy approach fits your specific pain profile—and how it should be monitored for safety.
Discussion